Development of the models for the analysis of the healthcare systems and pharmaceutical markets
Global healthcare spending growth will slow to 4.1%, despite rising costs, as governments start to assess the economic damage wreaked by the pandemic. Vaccinating the world against Covid-19 (coronavirus) will remain a core priority. However, healthcare systems will also need to start tackling a backlog of non-coronavirus care. Healthcare is not exempt from supply-chain problems, and governments will push ahead with regulation designed to increase resilience and lower costs. In 2022, the experts expect global pharmaceutical sales to increase by 4.6% in US-dollar terms (about half the rate seen in 2021, but still faster than that seen in most of the previous decade). The disruption suffered in 2020—when many countries were scrambling for medtech supplies—has died down, but the pharmaceuticals industry is still suffering the knock-on effects of the broader logistics crisis. During 2022 the EU and US will push ahead with the reshoring initiatives they started last year, when supply-chain disruption underlined their reliance on China. The US will use the purchasing power of public healthcare schemes to favour medicines produced within the US. The U.S. spends more on health care as a share of the economy — nearly twice as much as the average OECD country — yet has the lowest life expectancy and highest suicide rates among the 11 nations.
Thus, it is important to develop models for the analysis of healthcare systems and pharmaceutical markets of the OECD and EU countries and reveal the countries which are leaders in the mentioned areas. In this thesis the purpose is to provide brief analysis of some approaches for the evaluation of healthcare systems and pharmaceutical markets by means methods of taxonomy, cluster analysis and econometrics.
Nowadays it is possible to find variety of the approaches for the modeling healthcare systems and pharmaceutical markets on the global, national and local levels. We consider briefly the results of some our studies concerning the analysis of the development of healthcare systems and pharmaceutical markets in the OECD countries and countries of the EU.
Let present the models for the evaluation of the development of healthcare systems in the different countries based on the application of taxonomy approach. In our previous work we analyzed the data on the OECD countries for the period 2000-2010 and this information was used for calculation of integrated parameters (Table 1) [1]. The following complex criteria were chosen: 1) I1- financing of national health care system; 2) I2 - the population provision by health care resources and services; 3) I3 - indices of national health care system activity; 4) I4 – mortality rate of the population; 5) I5 – the population life expectancy; 6) I6 - the population health state on the basis of a self-estimation.
The integrated parameter values by criterion I1 were calculated with consideration for individual indices V1 - V4. For the analysis of the countries position by criterion I2 the individual indices X1 - X4 were used and for calculations of the countries positions by criterion I3 we used the individual indices P1 - P3. In order to determine the countries position with consideration for criterion I4, we used the individual indices D1 - D5, for criterion I5 – individual indices L1 - L3, for criterion I6 - individual indices M1- M3. For the calculations we used the OECD countries data with complete observations based on all criteria [1].
| Country | I1 | I2 | I3 | I4 | I5 | I6 |
|---|---|---|---|---|---|---|
| Austria | 0.562 | 0.652 | 0.538 | 0.652 | 0.836 | 0.765 |
| Belgium | 0.511 | 0.55 | 0.462 | 0.616 | 0.793 | 0.786 |
| Czech Republic | 0.279 | 0.572 | 0.503 | 0.402 | 0.536 | 0.646 |
| Finland | 0.42 | 0.484 | 0.227 | 0.69 | 0.794 | 0.639 |
| France | 0.555 | 0.479 | 0.456 | 0.667 | 0.931 | 0.715 |
| Germany | 0.574 | 0.713 | 0.557 | 0.668 | 0.806 | 0.587 |
| Hungary | 0.223 | 0.409 | 0.587 | 0.149 | 0.234 | 0.421 |
| Ireland | 0.44 | 0.326 | 0.264 | 0.536 | 0.841 | 0.891 |
| Korea | 0.202 | 0.278 | 0.119 | 0.691 | 0.838 | 0.265 |
| Mexico | 0.054 | 0.004 | 0.049 | 0.313 | 0.154 | 0.601 |
| Poland | 0.196 | 0.282 | 0.397 | 0.43 | 0.415 | 0.455 |
| Slovak Republic | 0.282 | 0.465 | 0.597 | 0.184 | 0.318 | 0.044 |
| Slovenia | 0.336 | 0.335 | 0.421 | 0.502 | 0.75 | 0.541 |
| Sweden | 0.482 | 0.385 | 0.299 | 0.697 | 0.882 | 0.835 |
| United Kingdom | 0.468 | 0.304 | 0.301 | 0.586 | 0.797 | 0.776 |
| United States | 0.602 | 0.288 | 0.272 | 0.576 | 0.617 | 1 |
The results showed that in 2010 the USA had the leading positions among other OECD countries by such criteria as: I1 - financing of national health care system (0.602) and I6 - the population health state on the basis of a self-estimation. Rather high positions by criterion I1 had such countries as Germany (0.574), Austria (0.562) and France (0.555). Mexico had the lowest position by criterion I1 (0.054). Such countries as Poland (0.196), Korea (0.202) and Hungary (0.223) also had low position by this criterion. Rather low positions by criterion I1 were also possessed by Slovakia (0.282) and Czech Republic (0.279). The best positions by criterion I2, the population provision by health care resources and services, belonged to Germany (0.713). Austria and Czech Republic also had rather high parameters by this criterion: 0.652 and 0.572 respectively. In comparison with other countries Slovakia also had rather good position with value 0.465. It was close to such countries as France (0.479) and Finland (0.484). Rather low positions by criterion I2 were marked for Poland (0.282) and Korea (0.278). The lowest position by criterion I2 was marked for Mexico (0.04). The highest parameters of health care system activity by criterion I3 were observed in Austria (0.538), Germany (0.557), and in the former socialist countries, such as: Czech Republic (0.503), Hungary (0.587) and Slovakia (0.597). By criterion I4 the best were positions in such countries, as: Sweden (0.697), Korea (0.691), Finland (0.69), France (0.667), and Germany (0.668). The lowest positions were marked in Hungary (0.149) and Slovakia (0.184) that testifies the unfavorable situation in these countries. So, by criterion I4 the position of Poland (0.43) and Czech Republic (0.402) were much better, than in Hungary and Slovakia. From the point of view of criterion I5 (life expectancy) the highest positions were occupied by France (0.931); Sweden (0.882); Ireland (0.841); Korea (0.838), Austria (0.836), Germany (0.801). The low positions by this criterion I5 were marked in Poland (0.415) and Slovakia (0.318). The lowest positions by criterion I5 were observed in Hungary (0.234) and Mexico (0.154).
By criterion I6, the population health state on the basis of a self-estimation, high positions were marked for the following countries: Ireland (0.891); Sweden (0.835); Belgium (0.786) and Great Britain (0.776). As mentioned before the leader by criterion I6 is the USA (1). In Slovakia the lowest position was marked by the given criterion. Thus, on the basis of the calculated values of integrated parameters by criteria I1- I6 the classification of the OECD countries was carried and leading position of the USA was revealed for criteria I1 and I6; according to the rest criteria the positions of the USA were not so successful.
Realization of other model was implemented on the data of 30 European countries according to the following system indicators: self-assessment of health (men) “good” or “very good” (% of total amount) (x1); self-assessment of health (women) “good” or “very good” (% of total amount) (x2); do not experience restrictions or discrimination in their usual activities due to health problems (% of the total amount) (x3); non-infectious morbidity and mortality (x4); ˗ the number of people with chronic diseases (% of the total quantities) (x5); child mortality (number of deaths per 1,000 healthy newborns) (x6); life expectancy (x7); expected life expectancy at birth (total) (x8); years of healthy life (women) (x9); years of healthy life (men) (x10); years of healthy life after 65 years (women) (x11); years of healthy life after 65 years (men) (x12). The results of the evaluation of socio-economic effectiveness of healthcare systems in the selected countries for 2020 is presented in Figure 1 [5].
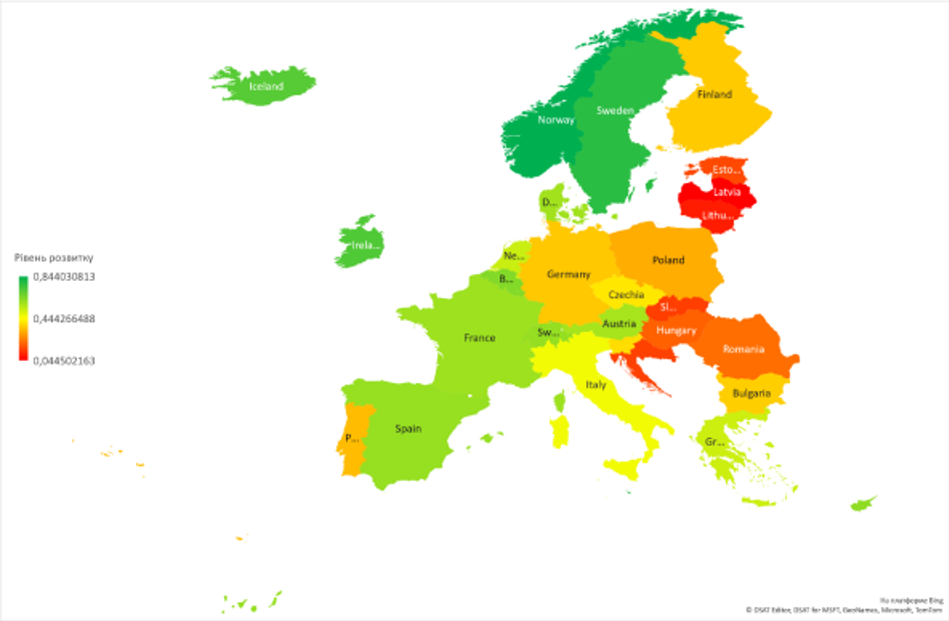
It is clear to see that for many European countries the results of the evaluation of socio-economic effectiveness of healthcare systems in 2020 are closed to the previous study of the national healthcare systems for 2010. Thus, the long-term gaps in the development of the national healthcare systems are observed and it can be explained by influence of many social, economic, political, emographical and environmental factors.
In other our paper we studied the features of financing national health systems in the EU-28 countries, and used such indicators as: TGEH1 (total government expenditure on health as % of GDP), TGEH2 (total government expenditure on health as % of total general government expenditure) and TGEH3 (total government expenditure on health per capita). For the description of the dynamics of the indicators such models as linear trend, exponential smoothing models (Holt’s models) were used [3].
For the grouping the countries of the EU-28 to reveal the regimes of funding healthcare systems we used data for period of 2000-2017 and k-means method of cluster analysis. It is should be noted that most of the EU-28 countries switched the regimes of the funding healthcare systems, it is proved that over period of 2000-2017 they moved from one kind of cluster to another one [4]. For most countries this switches from one type of cluster to another one occurred after long period, that it is possible to suggest the results of the economic development, new strategies of government, maybe after change of leading political party and other priorities in social or budget policies. Nevertheless, some countries demonstrated the stable policy in funding their national healthcare and over all period these countries were in the same cluster.
The national healthcare systems are related with level of the development of the pharmaceutical markets and we analyzed the main trends in the pharmaceutical markets in the world and in some macro regions and studied the development of the potential of leading pharmaceutical companies, which are among the TOP 1000 largest pharmaceutical companies in some regions (Eastern Europe, China, Middle East and Latin America) [2]. The largest medical and pharmaceutical corporations from the USA operate in many countries, provide and distribute progress in new medical technologies, equipment and treatment in modern hospitals and clinics worldwide. These corporations demonstrate impressive financial results and their securities are traded on the famous stock exchanges. Due to the dominate role of the 50 largest medical and pharmaceutical corporations in the USA it is possible to study the effect of Big Pharma and huge competitiveness in the global healthcare and pharmaceutical markets.
References
- Beňová E., Dubrovina N., Boyko V., Zamyatin P. Classification and cluster analysis of health care systems in the OECD countries / In: Verejná správa a regionálny rozvoj : Ekonómia a manažment.- Roč. X, č. 2 (2014), s. 45-56.
- Dubrovina N., Chemchykalenko R., Dubrovina V., Sanin S.Riven rozvytku potencialu farmaceuticnych kompanij-lideriv na prykladi rynkiv okremych regioniv svitu / In: National Health as Determinant of Sustainable Development of Society / Nadiya Dubrovina, Stanislav Filip.- Bratislava : School of Economics and Management in Public Administration in Bratislava, 2021.- p. 733-74.
- Dubrovina N., Gerrard R., Filip S., Dubrovina V. Modelling the trends of the healthcare funding in the EU countries / In: Przegląd Europejski.-Warszawa: Wydawnictwo Uniwersytetu Warszawskiego, 2021.- Vol. 2021, no. 1(2021), p. 61-80.
- Dubrovina N., Filip S., DubrovinaV. Classification of financial mechanisms of healthcare systems in the countries of European union / In: Recent Advances in Information Technology, Tourism, Economics, Management and Agriculture: Fourth International Scientific Conference ITEMA, 8 October 2020.- Belgrade: Association of Economists and Managers of the Balkans, 2020.- p. 169-176.
- Guryanova L., Dubrovina N., Sirotkina M. Modeli ocenki efektivnosti sistem zdravoochranenia / In: National Health as Determinant of Sustainable Development of Society / Nadiya Dubrovina, Stanislav Filip.- Bratislava : School of Economics and Management in Public Administration in Bratislava, 2021.- s. 721-732.